

by Catherine Forse MD FRCPC
March 30, 2026
Collagenous colitis is a non-cancerous condition in which inflammation develops in the lining of the colon. It belongs to a group of conditions called microscopic colitis, named because the changes that cause symptoms can only be seen when tissue is examined under a microscope — the colon looks entirely normal during a colonoscopy. The other main type of microscopic colitis is lymphocytic colitis, which is closely related and shares many features.
Collagenous colitis is not cancer and does not increase the risk of developing cancer. It is a chronic condition for many people, meaning it can persist or recur over time, but it responds well to treatment in most cases, and the outlook is generally good.
What are the symptoms?
The hallmark symptom of collagenous colitis is chronic watery diarrhea that can last for weeks, months, or years. The diarrhea can be frequent and disruptive to daily life. Other symptoms may include abdominal pain or cramping, bloating, fatigue, and unintentional weight loss.
Symptoms often come and go. Some people have prolonged flares followed by periods of improvement; others have more persistent symptoms. The severity varies widely from person to person.
Who is affected?
Collagenous colitis is more common in middle-aged and older adults, and it affects women significantly more often than men. It is one of the more common causes of chronic watery diarrhea in this demographic, though it is still relatively uncommon overall.
What causes collagenous colitis?
The exact cause is not fully understood, and it likely involves a combination of factors. Several contributing causes have been identified:
- Autoimmune reaction. The immune system appears to play a central role. Some researchers believe it may mistakenly attack the cells lining the colon, triggering ongoing inflammation.
- Medications. Certain drugs are strongly associated with collagenous colitis and may trigger or worsen it. The most commonly implicated include non-steroidal anti-inflammatory drugs (NSAIDs such as ibuprofen and naproxen), proton pump inhibitors (such as omeprazole and pantoprazole), and selective serotonin reuptake inhibitors (SSRIs, a class of antidepressants). If a medication is identified as a likely trigger, stopping it often leads to improvement.
- Changes in gut bacteria. Alterations in the normal bacterial environment of the colon may trigger an abnormal immune response in some people.
- Genetic factors. Some people may have a genetic predisposition that makes them more susceptible to developing microscopic colitis, though the specific genes involved are not yet well established.
In many cases, no single clear trigger is found, and the condition is managed based on symptoms rather than an identified cause.
How is the diagnosis made?
If your doctor suspects collagenous colitis based on your symptoms, they will recommend a colonoscopy — a procedure that uses a small flexible camera to look inside the colon. During the procedure, your doctor will take small tissue samples, called biopsies, from several parts of the colon. Taking biopsies from multiple locations matters because collagenous colitis can be patchy — it may affect one area of the colon. Still, not another, and a single biopsy from one site could miss the changes entirely.
In most cases, the colon looks completely normal to the camera during the colonoscopy. The diagnosis can only be confirmed when a pathologist examines the biopsies under a microscope and identifies the characteristic features described below.
What does the pathology report describe?
The pathologist looks for a specific combination of changes in the colon lining that together confirm the diagnosis of collagenous colitis.
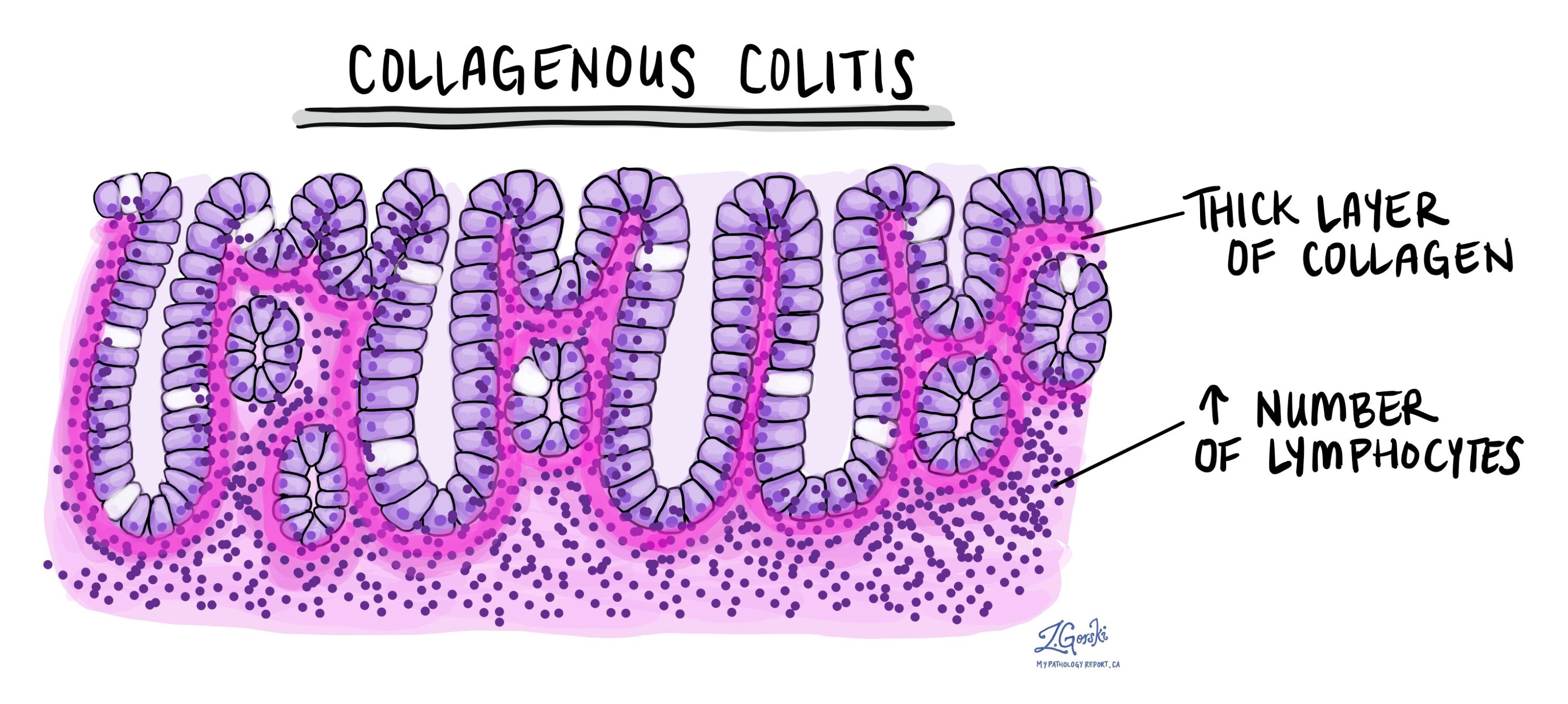
- Thickened collagen band. This is the defining feature of collagenous colitis and the reason for its name. Just beneath the surface layer of the colon lining, a band of collagen — a structural protein — builds up to an abnormal thickness. In a healthy colon, this layer is very thin and barely visible. In collagenous colitis, it thickens significantly and appears as a pale or pink band under the microscope. Pathologists sometimes use a special stain called Masson’s trichrome, which highlights collagen in blue or green, to confirm the finding. Tiny blood vessels and immune cells are often trapped within this thickened band.
- Intraepithelial lymphocytosis. An increased number of immune cells called lymphocytes is found within the epithelium, the surface layer of cells lining the colon. This is also the defining feature of lymphocytic colitis, which is why the two conditions share so many similarities.
- Increased immune cells in the lamina propria. The lamina propria — the thin layer of supportive tissue just beneath the surface — also contains an increased number of lymphocytes and plasma cells, indicating ongoing inflammation.
- Gland damage and atrophy. The glands (also called crypts) that line the colon can become damaged and shrink over time — a change called atrophy. Damaged glands produce less mucin, the substance that normally helps protect and lubricate the colon lining. This damage, combined with the thickened collagen band, interferes with the colon’s ability to absorb water properly and contributes to the watery diarrhea.
One important point: unlike ulcerative colitis and Crohn’s disease, collagenous colitis does not cause the serious structural damage — such as crypt distortion, ulcers, or abscesses — that is typical of inflammatory bowel disease (IBD). This distinction helps the pathologist confirm the diagnosis. It is also reassuring: the absence of those features means the colon has not sustained the kind of long-term architectural damage seen in IBD.
What happens next?
Collagenous colitis is a treatable condition, and most people experience significant improvement with appropriate management. The first step is to review any medications that may have triggered or worsened the condition. If an offending drug — particularly an NSAID, proton pump inhibitor, or SSRI — is identified, stopping it can lead to substantial improvement or even complete resolution of symptoms.
When medication adjustment alone is not enough, or when no medication trigger is identified, several treatments are effective:
- Budesonide. This is the most effective and most commonly used medication for collagenous colitis. It is a corticosteroid (a type of anti-inflammatory drug) that works locally in the colon with minimal absorption into the rest of the body, which reduces the side effects associated with typical steroids. Most people respond well to a short course of budesonide, though symptoms can return when it is stopped, and some patients require longer-term or intermittent treatment.
- Bismuth subsalicylate. Available over the counter, this medication (the active ingredient in products like Pepto-Bismol) can reduce symptoms in milder cases and is sometimes used as a first-line option.
- Cholestyramine. This medication binds to bile acids in the colon and can help reduce diarrhea in some patients.
- Diet and lifestyle adjustments. Some people find that avoiding caffeine, alcohol, dairy products, or high-fat foods helps reduce the frequency and severity of diarrhea. These measures do not treat the underlying inflammation but can help manage symptoms.
- Other medications. In more persistent or severe cases, a gastroenterologist may consider additional options, including immunosuppressants or biologic therapies.
Many people with collagenous colitis experience periods of spontaneous improvement, and some go into remission without active treatment. However, relapses are common, and ongoing follow-up with a gastroenterologist is important for managing the condition over time. Regular colonoscopies are not usually needed for surveillance, as collagenous colitis does not increase the risk of colorectal cancer.
Questions to ask your doctor
- Could any of my current medications be contributing to this condition?
- What treatment do you recommend, and how long will I need to take it?
- What should I do if my symptoms return after I finish treatment?
- Are there dietary changes that might help manage my symptoms?
- Will I need follow-up colonoscopies, and if so, how often?
- Is there anything about my case that would suggest a different underlying diagnosis?
Related articles
We are proud to partner with:
![]()