

by Jason Wasserman MD PhD FRCPC
February 25, 2026
Squamous cell carcinoma in situ of the oral cavity is a non-invasive cancer that affects the lining of the mouth.
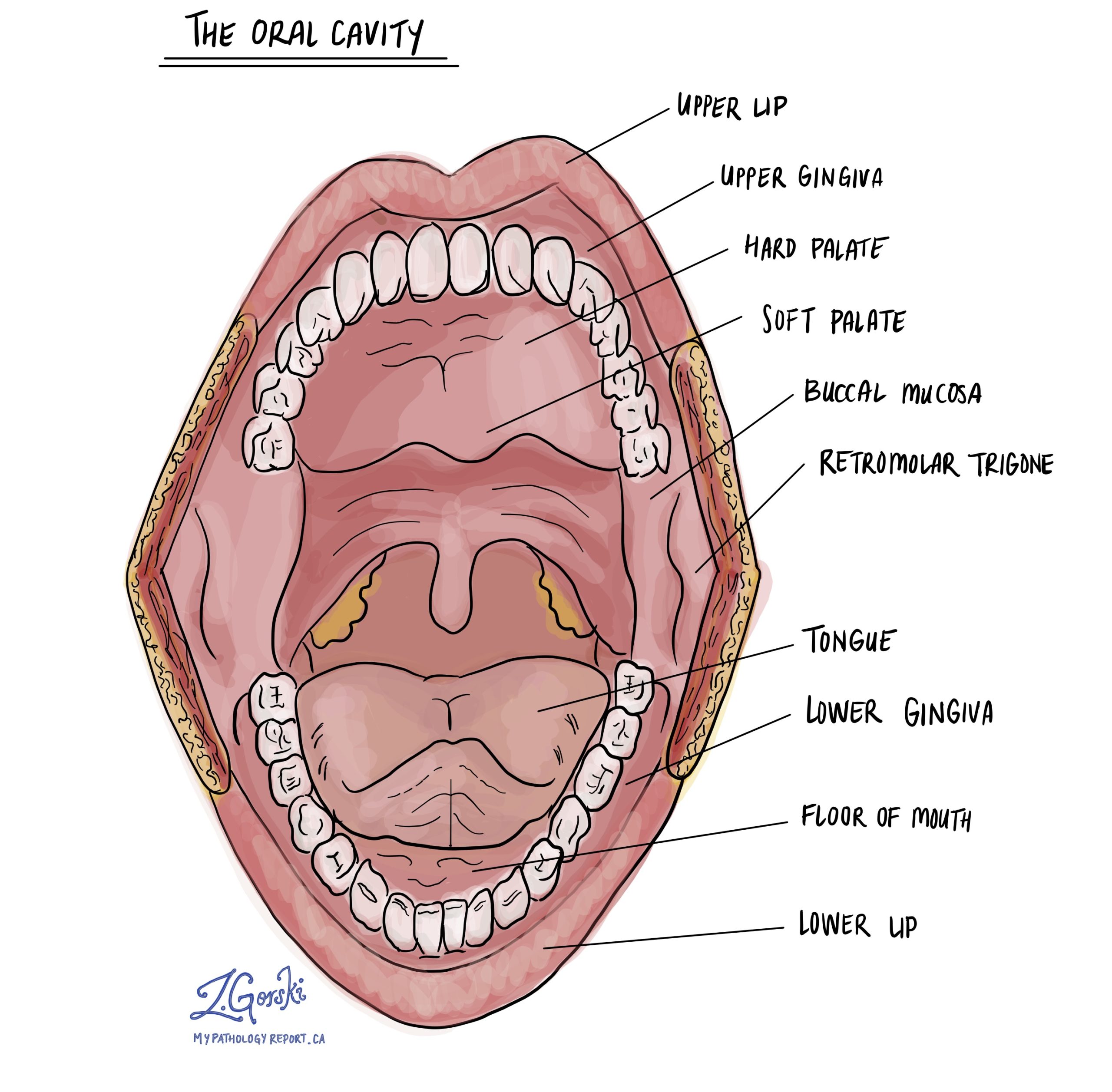
The oral cavity includes the lips, tongue, floor of the mouth, inner cheeks, gums, and hard palate. These areas are covered by a thin protective layer called the epithelium, composed of flat cells called squamous cells.
In squamous cell carcinoma in situ, the squamous cells exhibit severe abnormalities throughout the full thickness of the epithelium. However, the abnormal cells remain confined to the surface layer and have not invaded the deeper supporting tissue, called the stroma.

Because the abnormal cells have not invaded deeper tissues, this condition is called “in situ,” which means “in its original place.” Another name for this condition is severe squamous dysplasia.
Although squamous cell carcinoma in situ is non-invasive, it carries a high risk of progressing to invasive squamous cell carcinoma if left untreated.
Is squamous cell carcinoma in situ considered cancer?
Squamous cell carcinoma in situ is considered an early form of cancer because the cells show the same severe abnormalities seen in invasive cancer. However, it is considered non-invasive because the abnormal cells are confined to the epithelium and have not spread into deeper tissues.
Since invasion has not occurred, the cells cannot spread to lymph nodes or distant parts of the body. Once the tumor grows beyond the epithelium into the stroma, it is classified as invasive squamous cell carcinoma.
Why is it called “non-invasive”?
The term “non-invasive” means that the abnormal cells are located entirely within the epithelium.
The epithelium is separated from the deeper tissues by a thin barrier called the basement membrane. In squamous cell carcinoma in situ, the abnormal cells have not broken through this barrier. In contrast, invasive cancer occurs when tumor cells penetrate through the basement membrane and enter the underlying stroma, where they can access blood vessels and lymphatic channels.
What causes squamous cell carcinoma in situ?
The most common cause is tobacco use, including cigarettes, cigars, pipes, and smokeless tobacco. Tobacco exposes oral cavity cells to harmful chemicals that damage DNA and promote abnormal growth.
Heavy alcohol use also increases the risk, particularly when combined with tobacco. Alcohol weakens the protective lining of the mouth and makes it more susceptible to injury.
Other risk factors include immune suppression and chronic inflammatory conditions such as oral lichen planus. Long-standing irritation and inflammation can increase the risk of abnormal cellular changes.
What symptoms can occur?
Some people with squamous cell carcinoma in situ have no symptoms. Others may notice a persistent red patch, a white patch, or a mixed red-and-white area in the mouth.
The affected area may be painful, tender, or prone to bleeding. Because these changes can resemble noncancerous conditions, a biopsy is required to make the diagnosis.
How is this diagnosis made?
The diagnostic process usually begins when an abnormal area is seen during a dental or medical examination. A small tissue sample, called a biopsy, is removed and sent to a pathologist.
The diagnosis of squamous cell carcinoma in situ is made after microscopic examination of the tissue. In some cases, the diagnosis is made after the entire abnormal area is removed during an excision procedure.
Microscopic features
Under the microscope, squamous cell carcinoma in situ shows severe abnormalities affecting the full thickness of the epithelium.
The squamous cells are larger than normal and have enlarged, dark-staining nuclei. The nucleus is the part of the cell that contains genetic material. The cells often appear crowded and disorganized, and normal maturation from the bottom to the surface of the epithelium is lost.
Large nucleoli, which are small structures inside the nucleus, may be visible. An increased number of mitotic figures, cells actively dividing, is often observed. The abnormal cells may also show abnormal keratinization, meaning they produce keratin in an irregular pattern.
Importantly, the abnormal cells remain confined to the epithelium and do not invade into the underlying stroma.
What is the risk of developing invasive cancer?
If untreated, squamous cell carcinoma in situ has a high risk of progressing to invasive squamous cell carcinoma. Because of this risk, treatment to remove the abnormal area is usually recommended.
Early detection and complete removal significantly reduce the risk of progression.
What is a margin and why are margins important?
A margin refers to the edge of the tissue removed during surgery.
After the abnormal area is removed, the pathologist examines the margins under the microscope to determine whether squamous cell carcinoma in situ extends to the cut edge of the tissue.
A negative margin means that no abnormal cells are seen at the edge. This suggests that the lesion was completely removed.
A positive margin means that squamous cell carcinoma in situ is present at the edge of the removed tissue. This increases the risk that abnormal cells may remain in the body and that the condition could return at the same site. Additional treatment or closer follow-up may be recommended in this situation.
Questions you may want to ask your doctor
-
Was the entire lesion removed?
-
Were the surgical margins negative?
-
What is my risk of developing invasive cancer?
-
How often should I have follow-up examinations?
-
Are there lifestyle changes that could reduce my risk of recurrence?
We are proud to partner with:
![]()